
Displaying items by tag: policy
New FDA Consumer Update Urges Women to Obtain Medical Sonograms with Trained Operators
By Susan Dammann RN
The FDA has issued a warning. While the FDA's main focus in the warning is to advise pregnant women to avoid commercial sonogram services for nonmedical purposes that could pose a danger to the developing fetus, emphasizing that these are prescription medical devices, are to be used only by trained health care professional and only with a prescription, included within the warning are guidelines/recommendations which we in the pregnancy help medical clinics should be aware of.
Below are three excerpts from the 12/16/14 FDA Consumer Update which may pertain to the use of ultrasound imaging in the PMC, and a question for you to consider.
"Fetal ultrasound imaging provides real-time images of the fetus. Doppler fetal ultrasound heartbeat monitors are hand-held ultrasound devices that let you listen to the heartbeat of the fetus. Both are prescription devices designed to be used by trained health care professionals. They are not intended for over-the-counter (OTC) sale or use, and the FDA strongly discourages their use for creating fetal keepsake images and videos."
Question: Are the sonograms in your center being performed by trained health care professionals?
"The long-term effects of tissue heating and cavitation are not known. Therefore, ultrasound scans should be done only when there is a medical need, based on a prescription, and performed by appropriately-trained operators."
Question: Are the sonograms performed in your center based on a prescription for a medical need?
"Similar concerns surround the OTC sale and use of Doppler ultrasound heartbeat monitors. These devices, which are used for listening to the heartbeat of a fetus, are legally marketed as "prescription devices," and should only be used by, or under the supervision of, a health care professional."
Question: If your center uses Doppler, is it being used under the supervision of a health care professional?
As you consider the above FDA recommendations in relation to the ultrasound services performed in your PMC keep in mind also that one of the points in the Commitment of Care and Competence to which all Heartbeat Affiliates sign in agreement is:
Medical services are provided in accordance with all applicable laws, and in accordance with pertinent medical standards, under the supervision and direction of a licensed physician.
To read the full FDA Consumer Update click here.
When Others are Doing it Wrong

"Can you believe they're doing that?!"
"That's illegal. They can't do what they're doing!"
"Do they realize that what they do reflects on every one of us?!"
"They aren't following best practices!"
Yes, indeed others do it differently. Sometimes it's a difference of opinion and can be overlooked. Other times it might be a serious matter, possibly even a legal matter, which could threaten us all.
Or does it? Threaten us all, I mean.
We are, or should be, well-acquainted with threats, since they actually started happening the day each of us opened our doors (if not before). Our efforts to champion life are both defensive maneuvers and direct assaults on the kingdom of darkness, which tends to rile up our enemy a bit! It should come as no surprise when our enemy gets in on the action and stirs up those who oppose us – those who also happen to directly profit from or successfully rationalize their need for abortion.
When the opposition aligns with our enemy (please be careful not to assume the two are the same), the pushback on what we do (or who we are) is intense. And vicious. And nearly always without merit. The truth may be a great defense in the court of law, but attacks against us are mostly in the court of public opinion.
Actually, the number of legal actions against pregnancy help organizations is surprisingly small, considering the onslaught of relatively serious accusations including false advertising, impersonating a medical professional, and practicing medicine without a license.
This reality underscores the flaw in leaning too heavily upon legal principles to combat harsh, negative PR sound bites. To borrow a line from the movie Untouchables, it's a bit like bringing a knife to a gunfight.
The other side is serious about crippling our work, so they bring big weapons to the fight. Artful use of PR tools and political maneuvering is the only sustainable attack they have been able to use so far. The legal matters that concern us hardly concern them. If it did, they would have used the legal system to shut us down a long time ago. In fact, they've tried to do so, but found this strategy largely ineffective.
Instead, they've been launching state-by-state "Investigative Reports," badgering politicians to change the rules, manipulating the media to believing such things as Google pulling PHC ads and cyber-squatting on "crisis pregnancy center" entry in Wikipedia. And that's just the tip of the iceberg.
And what do we do? Well, we aim at each other for "doing it wrong."
We exert "legal expertise," passing along what we've heard labeled "illegal" without really knowing if it is actually, well, against the law. The old "telephone game" has us repeating, sometimes in directors meetings and public chatter, what someone else said they believe to be factual. Dare I say, some of what we believe is actually conjecture from well-meaning friendly lawyers (or those who pretend to be).
While we need to hear – and usually heed – advice from our legal allies, we must be careful to discern between recommendations and requirements, between what is permissible and profitable.
We can even exalt "best practices" – doing things "right" – above getting the mission done. Forgetting for a moment that most "best" practices are usually not proven to be "best" relative to our mission, we can tend to create the self-repudiating expectation everyone across the entire industry is operating at "best practice" level.
Believe it or not, the mission can actually be done without equipment or professionals or credibility. Just like the gospel. Of course, good equipment and education can (or should) enhance the effort. But when outcomes – hearts touched and lives saved – become subservient to so-called "best practices," we are all doing it wrong.
Tweet this! When outcomes become subservient to so-called "best practices," we're all doing it wrong.
Certainly the "others" might be able to do it better. Maybe they should have better equipment, more focused marketing and more professionals.
Or, maybe "they" are highly focused on outcomes, but just lack the resources to it differently. Maybe "they" are doing all they can, with what the Lord has seen fit to provide. Not every community has an abundant supply of pro-life, medical professionals ready to staff a pregnancy help center for a full week, plus weekends. Not just rural locations mind you, but some huge cities in certain blue states struggle with recruiting medical professionals.
Maybe the budget isn't big enough to fully meet AIUM standards, or voluntarily submit to HIPAA requirements, or afford the ultrasound equipment for which any of that might (notice: might) matter. Maybe "they" counsel and hand out material aid for the very purpose of interacting with at-risk women in a caring and compassionate way. Sometimes "their" method is wrongly assumed to reflect a desire for pregnancy support alone and not intervention services.
It's all too easy to judge from a distance and, without really understanding their circumstances and assume that what "they" are doing is wrong. But, let's remember what happens when we assume.
Let's also remember Proverbs 18:17, "The first person to speak always seems right until someone comes and asks the right questions." (ERV)
by Jor-El Godsey, Vice President
Fuss about Practice Fusion?
By Jor-El Godsey, Vice President
If you don't know the difference between EHR and EMR and PHR, HIPAA and HI-TECH, EPM and PMS , PRC and PMC, then stop reading.
If you do, or think you do, you're probably knee-deep in medical clinic regulations and/or clinic practices.
Pregnancy help medical clinics have been growing in number and complexity for the last twenty years. Originally focused on ultrasound services, many life-affirming, medically savvy centers are expanding medical services to include STI testing/treatment, pre-natal care, and more.
Good business systems, important for all pregnancy help organizations, has been a dynamic question for medically focused affiliates with the changing nature of health care regulations.
Life-affirming friends like eKyros and WayCool that specialize in database solutions for pregnancy help organizations have been answering that question with increased security, encrypted records and other HIPAA-necessary implementations. However, some in our community have either opted for, or promoted other software.
One of those is Practice Fusion. And, yes, there has been a fuss about Practice Fusion.
Practice Fusion is presented as being "free" (always attractive to non-profits) and, despite its relative newness (launched in 2007), has been quickly accepted by doctors office across the U.S. There are, however, some troubling findings that ought to give life-affirming pregnancy help organizations pause.
First, is anything really "free"? The article, "What Makes Free EHRs Expensive in the Long Run?" rightly notes, "...hidden expenses, heightened risk and unforeseen liabilities can cost you just as much as any web-based EHR..." So always beware of any Open Source product being offered for FREE.
Second, venture capitalists have invested nearly $200 million in this product. How will they realize their return on investment? It's always good to look a little closer to understand how a free product is able to remain current, supported and adaptable for future innovation. An article from Business Week notes the following:
The company makes money by charging more than 70,000 pharmacies, 300 diagnostics labs, and 21 imaging centers for access to its captive community of medical pros. For example, labs pay for the convenience of transmitting test results rather than faxing them, while drugmakers pay to deliver targeted ads to doctors. For an additional fee, companies can use a Practice Fusion tool to sift through its trove of more than 80 million patient records to identify patterns, such why doctors might be choosing one drug over another. The data is stripped of any information that would reveal the identity of the patients. The company is also working with insurer Aetna (AET) to identify at-risk patients to head off costly trips to the emergency room.
A pregnancy help organization using Practice Fusion apparently becomes part of the "captive community" targeted by those profiting from offering this "free" product.
Third, Practice Fusion's own practices have created significant compliance and confidentiality questions. Some industry watchers have noted, that "[a]ccording to experts, it may have violated the grand poobah of medical privacy laws — HIPAA — potentially getting both the doctors and Practice Fusion — as a "business associate" — into trouble. Additionally, the Federal Trade Commission may see what the start-up did as a deceptive business practice."
Along with these three specific points about Practice Fusion (or free EHRs in general), there comes a much more basic question:
Is there value in working within our specialized world of life-affirming pregnancy help to sharpen a good tool for all of us to use?
We think so, and we encourage you to think carefully when considering such important business tools.
Ebola 101

by Susan Dammann RN, Medical Specialist
With the recent presentation of Ebola cases in the United States, many in the health care field, including pregnancy center staff, are seeking to learn more about the virus and even more so, if prevention measures should be put into place. This article is intended as a resource to help you achieve those goals.
Part 1 will familiarize you with information about the Ebola virus, risks of transmission, symptoms of Ebola infection, and the diagnosis and treatment of Ebola victims, not inclusive of hospital protocol. Part 2 will offer recommendations and tools from various sources your center may wish to use to develop guidelines and procedures to screen for and deal with possible Ebola carriers.
Part 1: Information
Ebola, also known as Ebola hemorrhagic fever, is a severe viral illness that is rare and can be deadly. It is caused by an infection with one of the Ebola virus strains. To date, there have been nearly 9,000 reported cases of infection with Ebola in Africa in the recent outbreak, with more than 4,000 of those cases resulting in death.
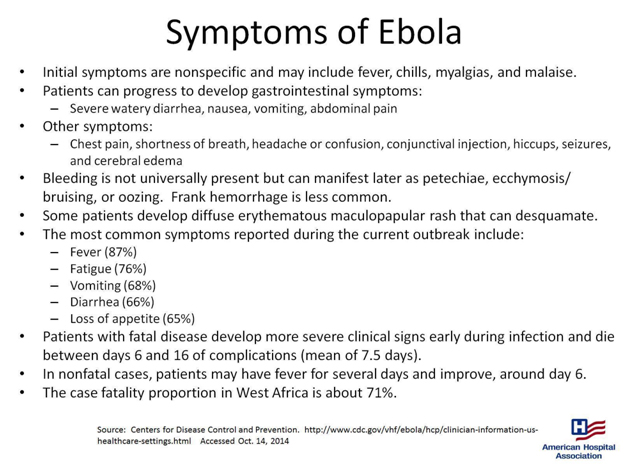
- "One of the difficulties in identifying potential cases of Ebola infection is the nonspecific presentation of most patients. Fever/chills and malaise are usually the initial symptoms, so all medical personnel should maintain a high index of suspicion in these cases.
- Patients who survive infection with Ebola generally begin to improve around day 6 of the infection.
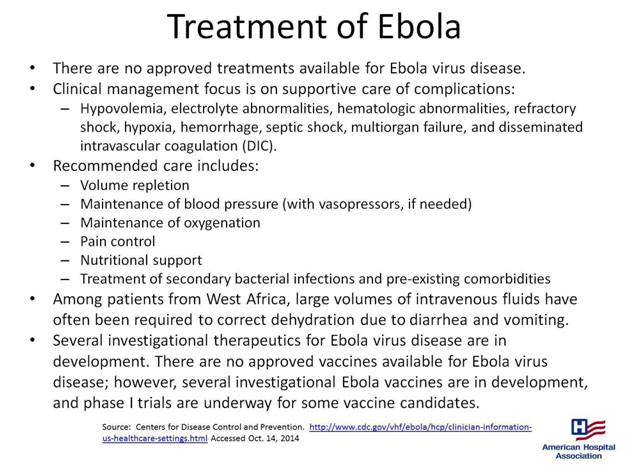
- There is no cure for Ebola infection; treatment is largely supportive. Therefore, prevention of the spread of Ebola in healthcare facilities is particularly important.
- Patients with fever, even subjective fever, or other symptoms associated with Ebola infection along with a history of travel to an Ebola-affected area within the past 21 days need to be identified in triage.
- If such a patient is identified, she/he needs to be isolated immediately in a single room with access to a bathroom. The door to the room should remain closed." (quoted from MedScape.org)

Transmission
"When an infection does occur in humans, the virus can be spread in several ways to others. Ebola is spread through direct contact (through broken skin or mucous membranes in, for example, the eyes, nose, or mouth) with
- blood or body fluids (including but not limited to urine, saliva, sweat, feces, vomit, breast milk, and semen) of a person who is sick with Ebola
- objects (like needles and syringes) that have been contaminated with the virus
- infected fruit bats or primates (apes and monkeys)
Once someone recovers from Ebola, they can no longer spread the virus. However, Ebola virus has been found in semen for up to 3 months. Abstinence from sex (including oral sex) is recommended for at least 3 months. If abstinence is not possible, condoms may help prevent the spread of disease."
(quoted from cdc.gov)
"Persons who have direct contact with infected individuals or their blood and body fluids, such as healthcare personnel without access to appropriate personal protective equipment or other caregivers in hospitals or homes, and persons handling bodies of deceased EVD patients are at high risk for Ebola virus exposure and infection.
Airborne transmission of Ebola virus has been hypothesized but not demonstrated in humans. While Ebola virus can be spread through airborne particles under experimental conditions in animals, this type of spread has not been documented during human EVD outbreaks in settings such as hospitals or households.
CDC infection control recommendations for U.S. hospitals, including recommendations for standard, contact, and droplet precautions for general care, reflect the established routes for human-to-human transmission of EVD and are based on data collected from previous EVD outbreaks in Africa in addition to experimental data."
(quoted from cdc.gov)
Can Ebola Be Transmitted Through a Sneeze?
"The only time that Ebola is in the lungs in sufficient quantities to produce virus in fluid that would be expelled during a sneeze is during extraordinarily advanced disease. A typical Ebola patient doesn't have a lot of virus in the lungs, but a person with advanced disease who is close to death could have a lot of virus in the lungs. During intubation, or when a very sick, infected person coughs or sneezes, an improperly protected healthcare worker could be at risk for being infected.
It would be a stretch to say that someone who is infected but well enough to walk around among other people would have enough Ebola in his or her lungs to be able to spread it by sneezing."
(quoted from MedScape.org)
Part 2: Recommendations and Tools
Pregnancy Center Considerations
If your center is currently serving clients from West African countries where the Ebola Virus has been reported, then you may wish to consider proactively creating a screening policy.
Should Ebola become a serious concern in our nation, the following are recommendations from various sources. Your board of directors in conjunction with your Medical Director or Medical Advisor may then need to develop the best strategy for your center in screening for Ebola carriers and what protocol your center will follow should such a person be identified.
Medscape interviewed Arjun Srinivasan, MD (CAPT, USPHS), Associate Director of CDC's Division of Healthcare Quality Promotion, asking some key questions about the Ebola crisis. They began with the upcoming influenza season and the worries that primary care clinicians may have about symptomatic patients who also have concerns about Ebola.
"Medscape: How should clinicians handle patients who present with symptoms of fever, nausea, and vomiting, in light of current Ebola recommendations?
Arjun Srinivasan, MD (CAPT, USPHS): It's important to remember that the telephone can be one of the tools that can help keep us safe from Ebola. When people call for appointments, it's an opportunity to ask them the screening questions about whether they might have risks for Ebola. Important in that is a travel history or potential exposure to a patient with Ebola. A checklist for patients being evaluated for Ebola is available on the CDC website.
Medscape: If there is no positive travel or exposure history in the past 21 days, can a clinician rule out Ebola?
Dr Srinivasan: Yes. The exposure or travel history is a key to identifying patients who might be infected with Ebola. There is an algorithm you can use to help you determine who might be at risk for Ebola, available at cdc.gov."
(quoted from MedScape.com)
The CDC Checklist for Patients Being Evaluated for Ebola Virus Disease (EVD) in the United States (linked to above) may offer some initial steps upon arrival of a possible carrier and initial assessment.
Below are three protocols and a questionnaire from the Franklin County, Ohio Health Department website. (Heartbeat International is located in Franklin County, Ohio) You may also want to look on the health department websites in your county for their recommendations.
Protocol for Assessing Possible Ebola Exposure in Healthcare Settings
Protocols for Dispatch and First Responders to Limit Exposure to Ebola
Protocol for Assessing Possible Ebola Exposure in Work Settings
Travel History and Exposure Screening Questionnaire
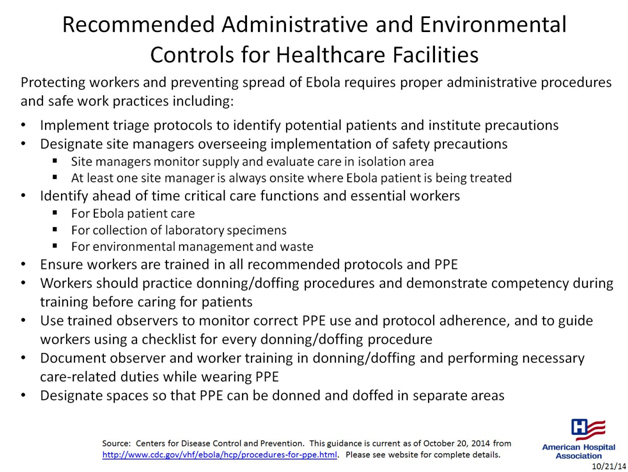
From the following document by the American Hospital Association the following may be of importance:
- Implement triage protocols to identify potential patients and institute precautions
- Designate site managers overseeing implementation of safety precautions
.
The following statements from the CDC may be helpful as you consider what steps to take.
"When a patient possibly infected with the Ebola virus appears in a hospital emergency department (ED), clinicians need not necessarily cover themselves from head to toe with personal protective equipment (PPE), according to new guidelines from the Centers for Disease Control and Prevention (CDC).
The CDC also emphasizes that ED patients with an unconfirmed Ebola infection are not contagious unless they are vomiting, bleeding, having diarrhea, or otherwise producing body fluids associated with an advanced stage of the disease and a healthcare worker comes in direct contact with them.
"If you're not at risk of being exposed to blood or body fluids, then you're not at risk of transmission," said Arjun Srinivasan, MD, associate director of the healthcare-associated infection prevention programs of the CDC's National Center for Emerging and Zoonotic Infectious Diseases. "When that risk exists — the patient is throwing up, for example — then you choose PPE that provides full-scale protection."
The first step in the CDC's algorithm for ED clinicians is determining the patient's exposure history: Has he or she lived in or traveled to a country with widespread Ebola disease or had contact with an infected person in the previous 21 days? If so, then the identification of Ebola signs or symptoms comes next. One sign is fever, either subjective or 100.4°F and higher. Other signs include headache, weakness, and muscle pain, as well as the red-alert symptoms of vomiting, diarrhea, abdominal pain, and hemorrhage, as in bleeding gums or nose bleeds.
A patient with these signs and symptoms along with a definite exposure history should be isolated immediately, either in a private room or a separate enclosed area with a private bathroom or a covered bedside commode. The CDC guidance states that only essential healthcare workers with designated roles should care for the patient and should log in and out of the room.
More information on the new Ebola guidance from the CDC is available on the agency's website.
(quoted from MedScape.com)
For additional or ongoing information, the CDC has a wealth of information available here.
Above all, we must look in faith to God Almighty for His wisdom and protection. Psalm 91 is a magnificent promise of protection and there is no better time for daily meditation in this Psalm, as we rest in faith in the One who is able to keep us safe in times of trouble.
The Best of Practices
By Jor-El Godsey
Remember when calling a center “Crisis Pregnancy Center” represented a widely accepted “best practice”?
Best practices, as defined at BusinessDictionary.com, are “methods and techniques that have consistently shown results superior than those achieved with other means, and which are used as benchmarks to strive for.” PRC’s have adopted varied practices over the years. Some flowed from moral or ethical considerations, others were informed by results or intuition. Hopefully, positive results followed all these practices. But have all these practices been subjected to rigorous comparison to “other means”? That is a critical step to specifically defining a best practice.
Any packaged “best practice” should be evaluated in light of the overall mission. This should include understanding the client who is the mission’s target, as well as the vision of the organization and its own definition of success. Variations between organizations, even programs within organizations, suggest that some, perhaps, many practices can’t be applied in the same way from organization to organization with the same effectiveness.
Best practice is more often a high-sounding buzzword for promotional material than an objective, empirical reality. It’s vital to analyze the foundation of any claim involving a best practice. For example in focus testing of the name “Crisis Pregnancy Center,” our target clients’ responses were weak. As a result, the term “crisis” has largely been eliminated from elements of client marketing in favor of new language with broader appeal.
Practices can certainly be good, effective, productive, healthy and even excellent. In time, these may even prove to be best! Until that time, some practices are really just common sense, conventional wisdom, and even basic standards.
Insurance FAQs
Why is insurance important?
- Insurance is a protection against loss, especially catastrophic loss, should something negative happen. Quality insurance is necessary to protect the organization, board members, staff and volunteers. Insurance, when needed, helps restore damage to resume serving and fulfilling the mission
What are key insurance products to look for when selecting insurance coverage?
- General liability (theft, slip and fall).
- D&O (Directors’ and Officers’ Liability) to cover the cost of defending against a legal action or the possibility of personal liability, especially related to hiring and firing of employees.
- Professional liability that covers staff, including peer-counselor and volunteer liability.
- Liability coverage for medical personnel, if you are a clinic.
- Cyber-security is increasingly important to consider.
What are Standing Orders and Are They Legal?
By Martha L. Teter MS, CRNP
 |
Many states in the United States have laws and rules regarding the use of “standing orders” or protocols for non-prescribers to administer medications. Do you know what the laws in your state are? Heartbeat International strongly recommends that you research your state laws in this area and be sure you are in compliance with them if you are operating in any area according to standing orders for the administration of treatment or medication, such as in the area of STD/STI treatment.
As an example, in the State of Ohio, no medication may be given to any patient without prior assessment of the patient’s condition by a legal prescriber and documentation of the legal prescriber's order on the patient's record.
Legal prescribers in the State of Ohio, include Physicians, and the following Advanced Practice Nurses who also hold Certificates to Prescribe: Certified Nurse Practitioners, Certified Nurse Midwives and Certified Clinical Nurse Specialists. Many Certified Physician Assistants also have Certificates to Prescribe and are legal prescribers.
A standing order or protocol is a definitive set of treatment guidelines that include definitive orders for drugs and their specified doses. These “Standing Orders” have been authorized by a prescriber to be administered by a certified or licensed health care professional, to a patient for a specific condition. This type of “Standing Order” or Protocol may only be utilized by licensed health care professionals in Ohio in the following situations.
- Emergencies
- Administration of biologicals for the purpose of disease prevention, and
- Administration of vaccines for the purpose of preventing disease
The administration of drugs for any reason other than the above exceptions and that are not patient specific or authorized by the prescriber prior to implementation would be the unauthorized practice of medicine, which is a felony in the state of Ohio. The details of how and when the above exceptions may be applied are detailed in Ohio law.
If you would like to learn more about Ohio Law regarding standing orders, click here.
Many other states also have laws regulating standing orders. To learn more about the laws in your state, log onto the professional websites of The State Board of Nursing, The State Board of Medicine or the State Board of Pharmacy. Should you find that your current practices are not in compliance with your state law, Heartbeat International recommends that you place a hold on further treatment until such time as you can assure you are in compliance with your state law.
If you have any further questions please feel free to contact Heartbeat International.
Developing a Thriving Team
 |
by Debra Neybert, Training Specialist
Since building an effective team will ultimately affect the women and men you are trying to serve, board members and directors looking to strengthen and nurture their team need to take specific steps to positively impact their staff and volunteers.
The Board of the organization is responsible for creating an environment that puts people first, that solves conflict in a healthy and biblical way, and that also allows people to develop and ultimately use their God-given gifts and talents to bless those they minister to.
A healthy leadership team (Board and Executive Director), can be a source of nourishment for an entire organization as they model servant leadership and provide professional development opportunities.
Pursuing Godly Servant Leadership
One characteristic of servant leadership comes prioritizing your relationship with the Lord, which then leads to pursuing a particular God-given mission. Board members should have a calling to follow the mission of your organization. The mission energizes and creates a passion for leaders to take on the responsibilities and jobs that come to Board members. It will also draw others to get involved and energize their passion for the mission.
Servant leaders should value their relationship with fellow members of the leadership team. These relationships must be characterized by love. In 1 Corinthians 13, the Apostle Paul describes the kind of love that God would have us exemplify. Servant Leaders are sensitive to the needs of those they work with (fellow leaders on the team), and to those under their direction. Servant leaders also lead by example and are willing to doing small jobs as gifts to others.
As the Cross drew near, Jesus introduced his followers to servant leadership as a radically new form of leadership, such that the world had never seen.
Jesus knew that the Father had put all things under his power, and that he had come from God and was returning to God; so he got up from the meal, took off his outer clothing, and wrapped a towel around his waist. After that, he poured water into a basin and began to wash his disciples' feet, drying them with the towel that was wrapped around him. (John 13:3-5)
Another characteristic of a servant leader is peace. It is always easy to remain peaceful when nothing is rocking your boat, but remaining peaceful is more challenging when struggles begin to surface, whether in relation to finances, personnel, internal or external challenges, transitions or attacks.
A peaceful environment is the result of effective servant leadership. This is an atmosphere of peacefulness that nourishes the organization when conflicts are handled in a biblical way. One extremely helpful resource Heartbeat recommends and uses is Ken Sande’s The Peacemaker: A Biblical Guide to Resolving Personal Conflict, a practical handbook for peacemaking based on Matthew 18. When this kind of conflict resolution is modeled by a leadership team, the entire organization benefits.
Cultivating a Professional Environment
Another way the Board can encourage and nurture its team is by proactively investing in professional development opportunities.
A good working environment is crucial, including space and equipment. It is the Board’s responsibility to see that those under their care, especially the Executive Director, are treated with dignity and respect. When dignity and respect are modeled, these virtues also filter down to the whole organization and bear much fruit.
A good salary and benefits for the Executive Director and staff are some of the ways that dignity and respect are shown, and it is always wise to plan ahead and make provision in the budget for continuing education and training for the Executive Director and staff.
Continuing education can be provided in many ways: through the Heartbeat Academy, one-on-one mentoring of the Executive Director by a Board member, community workshops provided by local foundations, a line item in the annual budget to send the Executive Director (and at least one Board member plus other staff and volunteers) to one of the Heartbeat International training events (Annual Conference, Executive Roundtable, Institute for Center Effectiveness).
A commitment to the on-site or online training of Board and/or staff every few years is also a tremendous way to nurture your center, while a prayer retreat for the Board and/or staff is a blessing that can be provided by a local pastor or priest (or both).
Training events also provide an excellent networking opportunity for Board Members and the Executive Director (and staff) with other nonprofits in the local community and, in the case of Heartbeat International events, with similar ministries all over the world.
Order Heartbeat International’s GOVERN WellTM today to find out how you can become a more effective leader in your life-affirming center.
Also, don’t let the chance to invest in your leadership excellence through the 2014 Heartbeat International Annual Conference, March 24-27 in Charleston, S.C.
Who is My Patient?
by Ellen Foell, Heartbeat International Legal Counsel
|
“A patient-physician relationship is generally formed when a physician affirmatively acts in a patient’s case by examining, diagnosing, treating, or agreeing to do so. "Once the physician consensually enters into a relationship with a patient in any of these ways, a legal contract is formed in which the physician owes a duty to that patient to continue to treat or properly terminate the relationship.” - Valarie Blake |

This sounds like a trick question a Pharisee might ask to entrap Jesus.
The answer seems fairly straightforward. The patient is anyone who receives medical services from a physician.[1] But then, there is a follow-up question: "When is my patient no longer my patient?" In other words, when does the legal obligation to the patient end?
The physician and the clients who walk through the center’s doors are indispensable to its existence as a medical pregnancy clinic. Without the client-patients, there would be no need for the medical center to exist. Without the medical director, the center has no legal authority to provide any of its critical life-changing medical services, including ultrasounds and sexually transmitted infection and disease testing.
The medical director’s presence in name, policy-setting, procedure, and writing standing orders creates a patient-physician relationship. It runs between the physician and every client who walks through your doors to receive medical service.
However, much like ambulatory care clinics, the relationship between the physician in a medical pregnancy center and patient is limited in time and treatment, so the center must set distinct parameters to avoid confusion for the patient and liability for the center. Failure of the center to be clear in setting and communicating those parameters to the patient can create liability-laden situations.
The best way for centers to avoid liability issues is to be up-front in communicating the parameters of the patient-physician relationship with each client. In the eyes of the law, the physician-patient relationship continues if the following three factors are present, with the third factor posing the most relevance for pregnancy help centers:
- The client-patient needs follow-up treatment from a physician,
- The client-patient has a reasonable expectation of continued treatment, and
- The physician has not clearly and explicitly ended the relationship.
It is easy to see how a client-patient could leave a center with the impression that she and the medical director have now established a continuous patient-physician relationship. Treatment and care for a pregnant woman typically involves multiple doctor visits, additional ultrasounds, and can include additional procedures as well.
Further, since many of the women coming to a medical pregnancy clinic may not have an existing relationship with a physician, a client-patient might naturally conclude that the relationship would continue beyond the parameters of that place (the center) and time (the appointment).
That is, the client-patient might have a reasonable expectation of continued services because she clearly requires continued treatment. The question is, “From whom?” That question can and must be addressed in the context of clear and explicit communication to the client that the patient-physician relationship is terminated upon her leaving the pregnancy medical clinic, and—if needed—receipt of referrals for obstetrician-gynecologists, in keeping with standard pregnancy medical center practice.
If the client is clearly and explicitly informed—verbally and in writing—that no continuing patient-physician relationship continues after the verification of pregnancy and/or ultrasound, then the center and its medical director will have fulfilled their legal duty to the client. In fact, most pregnancy medical centers have a Consent and Release Form for the client to sign, indicating this agreement.
Heartbeat International was recently asked whether giving a regimen of prenatal vitamins or prescribing prenatal vitamins constituted a continuation of the patient-physician relationship, possibly exposing the center to liability. The question was raised for obvious reasons: Prenatal vitamins tend to be something pregnant women take throughout the course of their pregnancy, implying continuing treatment.
Arguably, prescribing the vitamins could be interpreted to constitute action taken pursuant to the patient-physician relationship. Thus, a center will want to ensure that its Consent and Release Form is broad enough to encompass the prescription for vitamins.
Pregnancy help medical clinics daily provide excellent and caring life-saving services. In the event that a client-patient is pregnant, she should be given referrals for other service providers.
Centers should have an attorney draft a Consent and Release Form, which should be given and explained to the client-patient. This paperwork should clearly state that no follow-up care will be provided, and that the patient-physician relationship is terminated.
That form must be signed by both center staff and the client-patient, with a signed copy given to the client-patient and a copy kept in the client-patient’s medical file. In following these guidelines, a center will have fulfilled its obligation to the client-patient, and to the law.
Go and do likewise!
Tasking volunteers?
by Jor-El Godsey, Heartbeat International Vice President
 “Let’s get the volunteers to do it. That will save a bundle!”
“Let’s get the volunteers to do it. That will save a bundle!”
Volunteers are often seen as a supply of labor for almost any task or for the implementation of an action item. Leaders - board members and directors alike - often assume that volunteers are the least expensive option available. Think again.
Many moons ago, our pregnancy help center utilized a team of volunteers to accomplish the bulk mailing of our newsletters and appeals. Trays of printed material and envelopes along with stickers and labels were distributed. Presto, some two weeks later the mailing had been delivered.
Upon closer inspection, we realized that, in addition to the volunteer time, two staff members had spent ten work hours (a total of twenty staff hours) each mailing cycle to coordinate the assembly, distribution, and postal paperwork for this process. A local mailing service (also known as a fulfillment house) that had more sophisticated equipment could lower the postal rate and turn the same task around in three working days as opposed to two weeks. Cost comparisons revealed that, for just a few dollars more, we could improve our process, tighten our turn around, and release several volunteers to more personally rewarding tasks.
All leaders recognize the scarcity of resources to accomplish the mission and achieve the vision. The good leader continually evaluates how to allocate the limited resources available for maximum return on the investment for the ministry and those involved.
Adapted from DIRECT Well™, Heartbeat International’s manual for directors.
From On the LeaderBoard | Volume 2, Issue 2
