
Jennifer Wright
New FDA Consumer Update Urges Women to Obtain Medical Sonograms with Trained Operators
By Susan Dammann RN
The FDA has issued a warning. While the FDA's main focus in the warning is to advise pregnant women to avoid commercial sonogram services for nonmedical purposes that could pose a danger to the developing fetus, emphasizing that these are prescription medical devices, are to be used only by trained health care professional and only with a prescription, included within the warning are guidelines/recommendations which we in the pregnancy help medical clinics should be aware of.
Below are three excerpts from the 12/16/14 FDA Consumer Update which may pertain to the use of ultrasound imaging in the PMC, and a question for you to consider.
"Fetal ultrasound imaging provides real-time images of the fetus. Doppler fetal ultrasound heartbeat monitors are hand-held ultrasound devices that let you listen to the heartbeat of the fetus. Both are prescription devices designed to be used by trained health care professionals. They are not intended for over-the-counter (OTC) sale or use, and the FDA strongly discourages their use for creating fetal keepsake images and videos."
Question: Are the sonograms in your center being performed by trained health care professionals?
"The long-term effects of tissue heating and cavitation are not known. Therefore, ultrasound scans should be done only when there is a medical need, based on a prescription, and performed by appropriately-trained operators."
Question: Are the sonograms performed in your center based on a prescription for a medical need?
"Similar concerns surround the OTC sale and use of Doppler ultrasound heartbeat monitors. These devices, which are used for listening to the heartbeat of a fetus, are legally marketed as "prescription devices," and should only be used by, or under the supervision of, a health care professional."
Question: If your center uses Doppler, is it being used under the supervision of a health care professional?
As you consider the above FDA recommendations in relation to the ultrasound services performed in your PMC keep in mind also that one of the points in the Commitment of Care and Competence to which all Heartbeat Affiliates sign in agreement is:
Medical services are provided in accordance with all applicable laws, and in accordance with pertinent medical standards, under the supervision and direction of a licensed physician.
To read the full FDA Consumer Update click here.
IUD Usage in Adolescents
by Marilyn Henderson, RN Freda M. Bush, MD
Medical Institute for Sexual Health
Website: www.medinstitute.org Email: This email address is being protected from spambots. You need JavaScript enabled to view it.
A recently released policy statement by the American Academy of Pediatrics encourages Pediatricians to counsel adolescent patients regarding contraception in order of effectiveness. The most effective contraception is the progestin implant and the second most effective device is the intrauterine device, or IUD. Historically, IUDs were not used in nulliparous women (those who had not previously given birth), nor in women outside of a monogamous relationship. The uterine cavity is usually larger in women who have already carried a pregnancy and it was believed that a smaller uterine cavity would not tolerate a foreign object well, expelling the IUD and increasing the risk of pregnancy. The concern for women who were not monogamous was the increased risk for sexually transmitted infections that could develop into pelvic inflammatory disease.
Additionally, patients who believe that life begins with conception, need to be counseled that although the chemicals included with the IUD (copper or progestin) are designed to inhibit sperm from reaching an egg, IUDs also affect the lining of the uterus, making it undesirable for implantation, if conception does occur.1,2 In addressing the concern of conception occurring with an IUD in place, the Technical Report of the Academy of Pediatrics simply skirts the issue like this:
"The primary mechanism of action of both types of IUD is preventing fertilization by inhibiting sperm motility. The levonorgestrel IUDs also thicken cervical mucus. All mechanisms occur before implantation, when pregnancy begins, and inhibiting implantation is not believed to be a primary mechanism of action for either type of IUD."3
The report does not leave room for personal opinions and beliefs about when pregnancy begins, but simply states that pregnancy begins with implantation. Since the copper IUD, Paragard, is approved for use as an emergency contraception, there is even more concern for those who view the IUD as an abortive method of birth control. Paragard is reported to be 99% effective in preventing pregnancy,4 if inserted up to five days following unprotected intercourse.3 Medical Institute's greatest concern for IUD use in teens is sexually transmitted infections, which can lead to pelvic inflammatory disease and infertility (the inability to achieve pregnancy when desired). This concern is addressed in most of the current literature, but is not seen as a contraindication for IUD use. Interestingly, the CDC's fact sheet on PID6 lists the following risk factors for PID:
- Have an STD and do not get treated;
- Have more than one sex partner;
- Have a sex partner who has sex partners other than you;
- Have had PID before;
- Are sexually active and are age 25 or younger;
- Douche;
- Use an intrauterine device (IUD) for birth control
Just being a sexually active teen is a risk factor for PID. When the IUD is inserted, a second risk factor is added. Another CDC Fact Sheet, "Sexually Transmitted Infections Among Young Americans", points out that "many young people have multiple sex partners", indicating that risk factors numbers 2 and 3 for PID might also be a concern. And finally, the Fact Sheet mentions that many infected teens are often unaware that they have an STI and have not had the proper screening for Chlamydia, indicating risk factor number 1. With five out of seven risk factors for PID specifically being a concern among teens, one must wonder about any recommendation for IUD use in youth.
The American Academy of Pediatrics Technical Report continues the mixed message with statements like this: "...past associations between infertility and IUD use among nulliparous women were attributable to STIs rather than IUDs"3(page e1262) and the CDC Practice Recommendations states, "Although women with STDs at the time of IUD insertion have a higher risk for PID, the overall rate of PID among all IUD users is low."5
The answer to the problem of STIs from both the CDC and the Academy of Pediatrics is condoms. Both organizations recommend that all patients be counseled on the use of condoms, regardless of their choice of contraception to help prevent STIs. However, in 2013, only 8.8% of sexually active high school students reported using condoms along with another method of birth control8, perhaps indicating that with the fear of pregnancy gone, there is little motivation to use condoms.
Fifty percent of all new cases of STIs occur in young Americans from 15–24 years of age. Ignoring the increased risk for PID and resulting infertility for the sake of preventing teen pregnancy is not in the best interest of our youth. Therefore, MI does not agree with the recommendation for IUD placement in adolescent girls.
References:
1). "ParaGard T380A Intrauterine Copper Contraceptive", Rev 6/2013, ParaGard – FDA prescribing information, side effects and uses, Retrieved Oct 2014 from Drugs.com, http://www.drugs.com/pro/paragard.html
2). Skyla (levonorgestrel-releasing intrauterine system, full prescribing information, Retrieved from website Oct. 2014, www.skyla-us.com
3). Ott Mary, et al, Committee on Adolescents, "Contraception for Adolescents: Technical Report," Pediatrics: Official Journal of the American Academy of Pediatrics, 2014;134;el257; originally published online September 29, 2014; DOI: 10.1542/peds.2014-2300. Retrieved Oct. 2014. (quote: p. e1262)
4). Belden P & Harper C, "The Copper IUD for Emergency Contraception, a Neglected Option," (Editorial), Contraception 85(2012) 338-339
5). CDC, "U.S. Selected Practice Recommendations for Contraceptive Use, 2013: Adapted from the World Health Organization Selected Practice Recommendations for Contraceptive Use, 2nd Edition," prepared by: Division of Reproductive Health, National Center for Chronic Disease Prevention and Health Promotion, Morbidity and Mortality Weekly Report, Recommendations and Reports/Vol.62/No.5, June 21, 2013. (quote: p. 10)
6). CDC, "Pelvic Inflammatory Disease (PID) – CDC Fact Sheet", Retrieved Oct 2014 at http://www.cdc.gov/std/pid/stdfact-pid.htm
7). CDC, "Sexually Transmitted Infections Among Young Americans", July 2014. Retrieved Oct 2014 from http://www.cdc.gov/nchhstp/newsroom/2013/SAM-Infographic-2013.html?s_cid=nchhstp-nr-sam-008
8). CDC, "Youth Risk Behavior Surveillance – United States, 2013," Morbidity and Mortality Weekly Report, June 13, 2014, Surveillance Summaries/Vol.63/No.
Reprinted with permission from the Medical Institute for Sexual Health: Marilyn Henderson, RN (1st Author listed) and Freda M. Bush, MD (2nd Author listed).
Ultrasound Safety – Revisited
by Kevin T. Rooker, RT(R), RDMS, RVT, Sonography Consultants
Is ultrasound safe? Will it hurt my baby? These are questions we sometimes hear from our clients. We need to be able to answer those questions with confidence for several reasons. First, because our patients deserve an honest answer, and second because we never know who is listening. We know that there are some that think you should not be performing limited OB ultrasound and will always be looking for reasons to justify their position. Let's not give them that opportunity on the issue of ultrasound safety. Unfortunately, we, the medical community, have not done as well as we can at educating ourselves on the safety of ultrasound1.
Ultrasound is a wave of mechanical energy that penetrates human tissue as an oscillating (alternating) wave of high and low pressure. As it does so, there are two potential types of biological effects; Mechanical and Thermal. In 1993, the FDA allowed ultrasound manufacturers to significantly increase the amount of ultrasound energy created in diagnostic ultrasound systems, as long as they displayed the MI (Mechanical Index) and TI (Thermal Index) on the screen for the operator (and our clients) to see. The premise being that if we know what the MI and TI are, what their limits are, and most importantly how to lower them, then we are being as safe as we possibly can.
The Mechanical Index is a safety metric which lets the operator know how much energy is being transmitted into the patient during a sonography examination. Remember that sound is created by pressure waves, so mechanical energy is transmitted into any object which receives sound. Sound waves can be quite powerful. For example, think of the thump on your chest when sitting next to a teenager's car with the high dollar stereo system. It is defined as the peak negative pressure (PNP) of the ultrasound wave (point of maximal rarefaction). In easier terms; think pressure change divided by time. Lots of pressure change over short periods of time can be damaging. The FDA has established a maximum MI of 1.9 for diagnostic imaging. Any machine capable of generating MI greater than 1.0 must display the MI onscreen. The FDA MI limit for obstetric sonography is 1.0.
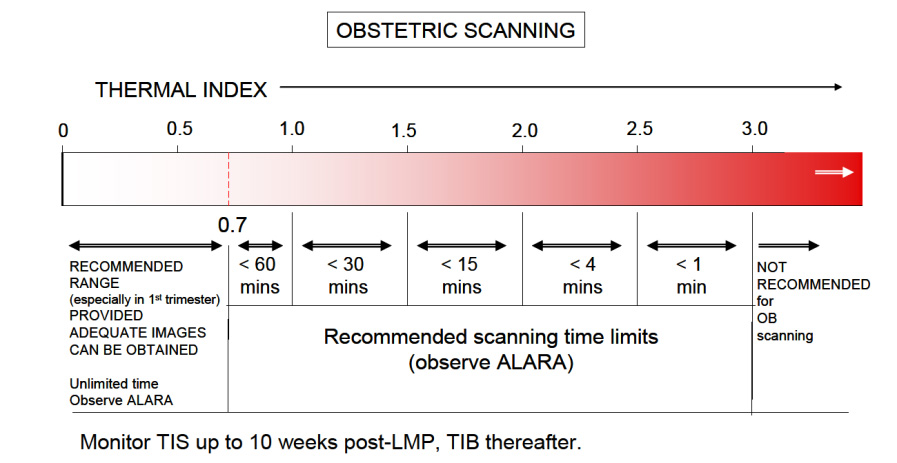
The Thermal Index is another safety metric which lets the operator know the potential of creating heat (hyperthermia) with the ultrasound beam. Many assumptions are made in this calculation, and it is often thought that the heating potential is underestimated. So keep in mind that the TI formulation was not intended to, and cannot provide an accurate measure of temperature rise within a specific patient. Instead it was designed to provide the operator with a relative measure of risk for a particular imaging mode. A Thermal Index of one (TI 1) indicates conditions under which the rise in temperature would be likely to be 1°C. The thermal index is different for different types of tissue, and can be displayed on your system accordingly: soft tissue (TIs), bone (TIb) and cranium (TIc). In the first trimester, when using Doppler to hear and demonstrate the fetal heart, the TIs setting us used. The limit for TI varies with time, please reference the chart below from the British Medical Ultrasound Society, the entire document may be found here.
Enough about what the MI and TI are, how do we as operators keep them at safe levels? There are two basic concerns to remember.
First is the AIUM ALARA policy2; which is an acronym for As Low As Reasonably Achievable. Simply translated, it means to keep the output power settings as low as possible, that still allows for adequate images. Most ultrasound systems can operate with output power settings at about 50% and still produce quite satisfactory OB images. Have your system presets adjusted so that when you are performing OB sonography both (abdominally and transvaginally), the output power settings are set low. You can always increase them if clinically necessary. And keep in mind that you can increase the gain to make your image brighter, as gain is just how well the system is "listening", it has no effect on the TI.
The second concern is time. Keep the overall examination as short as is reasonable. If using Doppler to allow Mom to hear her baby's heartbeat, depending upon your ceter's policy, keep the Doppler exposure to about 5-10 seconds. Know where to find the MI and TI displays on your system. If you don't know, consult your operator's manual or contact the manufacturer of your ultrasound system for more information.
Diagnostic ultrasound in obstetrics has been around for the better part of 40 years. To date, no one has been able to prove (and many have tried) that diagnostic ultrasound, when used prudently (MI,<1.0 and TI<0.7), has had any adverse effects developing fetuses; and this includes the limited use of Doppler in the first trimester "Thus far, there have been no significant thermal effects documented in humans and at this time the possibility of having all the factors present to is highly unlikely 3." However, it has been shown that aborting a living fetus is fatal, every time.
References
1. Ultrasound Is Safe . . . Right? Resident and Maternal-Fetal Medicine Fellow Knowledge
Regarding Obstetric Ultrasound Safety. J Ultrasound Med 2011; 30:21–27
Sheiner E, Abramowicz JS. Clinical end users worldwide show poor knowledge regarding safety issues of ultrasound during pregnancy. J Ultrasound Med. 2008;27(4):499-501
2. As Low As Reasonably Achievable (ALARA) Principle Approved 4/2/2014 aium.org/officialStatements/39
3. FDA Recommendations for the Safe Use of Ultrasound in Obstetrics CNE article authored by Sherri A. Longo, M.D. Assistant Professor in the Department of Obstetrics and Gynecology, Division of Maternal-Fetal Medicine, Tulane University School of Medicine in New Orleans, Louisiana; e-edcredits.com/nursingcredits/article.asp?testID=29
Positive Pregnancy Center Resolutions Sweep the Country
By Jeanneane Maxon, Vice President of External Affairs and Corporate Counsel, Americans United for Life
Attacks against pregnancy centers across the country have been widespread, and many of you have personally experienced them. In recent years, over a dozen states and localities have considered legislation promoted by NARAL designed to drive clients away from pregnancy centers and the life-saving help you provide.
Such bills typically include ridiculous requirements, such as disclaimers like, "This center is not required to provide you factually accurate information." In many instances, centers would be required to include such inaccurate and burdensome disclaimers in all client advertising, sometimes in 24 point font, and in Washington State, in five languages including Laotian.
If this sounds absurd to you, you are not alone. Every court that has had to consider such legislation has found it to be not only absurd, but unconstitutional. In fact, just this year, a court found an anti-pregnancy center ordinance imposed by Montgomery County, Maryland to be so inappropriate that it ordered the county to pay $375,000 in attorney's fees, costs, and nominal damages to the plaintiff pregnancy center.
Although they have been successful, efforts to defend pregnancy centers have cost time, energy and critical focus away from the women you serve. As Christian ministries, pregnancy centers should be strategic and prepared to defend themselves in the most efficient ways possible. We are called to be as wise as serpents and as gentle as doves. "I am sending you out like sheep among wolves. Therefore, be as shrewd as snakes and as innocent as doves." Matthew 10:16. Proactive efforts, therefore, should be bathed in prayer and approached with strategic steps to make victory come easier.
As one strategy to shield these attacks, Americans United for Life (AUL) drafted a Joint Resolution Honoring the Work of Pregnancy Resource Centers which provides state legislators, as well as county and city officials, an opportunity to praise pregnancy centers. In 2010, following the launch of state-based attacks in Oregon, AUL published this resolution and began working for its passage.
To date, 23 Pregnancy Center Resolutions have been passed in 17 states (some states passed the resolution in multiple years) including Alabama, Arizona, Florida, Georgia, Kansas, Missouri, Nebraska (by way of a "proclamation"), New Hampshire, Oklahoma, South Carolina, South Dakota, Tennessee, Texas, Utah, Virginia, West Virginia, and Wisconsin. Currently a resolution is also under consideration in Ohio.
As a first benefit, the resolution gives PRCs the ability to publicly highlight the work they do for their community. When a resolution passes, pregnancy center directors and volunteers are often invited to the statehouse and photographed with the Governor and/or significant government leaders. Additionally, many states also provide copies of the resolution for the center suitable for framing and display. Such an endorsement adds credibility in the minds of donors, clients and other influencers.
Additionally, when pregnancy centers are praised by a state or representative body of the people, the attacks on pregnancy centers lose credibility. For example, in 2010, Virginia legislators were so appalled by harassment NARAL inflicted on pregnancy centers through hostile legislation attempts, that they not only refused to enact NARAL's legislation, but turned around and passed the resolution praising the centers two weeks later.
Likewise, West Virginia has been on the forefront supporting the work of their pregnancy centers by way of a resolution. This state has consistently honored pregnancy centers every year since 2011. In 2012, the resolution became particularly meaningful when a hostile state legislator inappropriately wrote a letter to all the pregnancy centers demanding they supply him with confidential center files for a make-shift unofficial "investigation."
The pregnancy centers were able to respond simply by reminding this official that both the West Virginia House of Representatives and Senate had passed the resolution praising pregnancy centers for their outstanding service to the State and their communities. Presumably in embarrassment, the legislator stopped his harassment campaign and nothing more has been heard from him.
The impact of these resolutions is so profound that Heartbeat International and AUL believe that every pregnancy center should have a resolution passed in their state.
We can assist pregnancy centers in doing so. Pregnancy Center Action kits (with tools and instruction on passing the resolution) will be available to pregnancy centers in February, and the resolution and its corresponding policy guide is currently available at http://www.aul.org/legislative-resources/order-model-legislation/ (select Joint Resolution Honoring Pregnancy Resource Centers), or by contacting AUL at 202-741-4901.
We are privileged to stand by pregnancy centers that are doing the frontline work of helping women choose Life for themselves and their unborn children. We pray that this work carries on, uninhibited, until all are welcomed in life and protected in law.
Learning Together . . . without the Travel!
by Jennifer Minor, Editor/Writer
Somewhere between Pregnancy Help Institute and the Heartbeat International Annual Conference every year, there's a training gap. Individuals continue to take courses online at Heartbeat Academy, but that communal learning experience is missing.
That's why Heartbeat International developed ConCERT.
ConCERT is an advanced distance learning course to equip volunteer consultants with the information, skills, and perspectives that take them to the next level for providing effective consultation to individuals making choices in regard to sexual integrity, pregnancy, and parenting.
Deb Neybert, MA, LAS says, "As a trainer, I enjoy getting to know the students, and reading their comments posted on our online forum. Often they have great insights to share with each other, and it enhances the learning experience."
Since The LOVE Approach training is a pre-requisite to ConCERT, students interact with peers that have had similar experiences. According to Neybert, "Students say the most exciting part of ConCERT is the practical application as they have the opportunity to respond to verbatim assignments and the on-line forum communication."
Besides all of these benefits, by the end of ConCERT, students earn 14 CEU's toward the Life Affirming Specialist Designation. That's enough to apply for or renew your LAS!
Tweet this! The next session of ConCERT begins on January 11, 2015, and registration is open now.
The next session of ConCERT begins on January 11, 2015, and registration is open now. Information on pricing, registration, and other important dates can be found here.
Learn more and sign up today!
The Case for Support: Hardly a "Boring" Document!
by Kirk Walden, Advancement Specialist
Tweet this! When I think of what we call a "Case for Support" I yawn just uttering the words.
When I think of what we call a "Case for Support" I yawn just uttering the words. Couldn't we have come up with a better name for the very document that should convince our friends to join us in a mighty endeavor that could literally change history?
If you are wondering, a Case for Support, by definition, is a document whereby a ministry gives a "case" for why a particular initiative, or the ministry in general, deserves financial backing from a particular person, or the community at large.
But I'm going to be direct here: The terminology is boring.
Consider, if your ministry has a bold initiative that will save lives and change lives forever . . . This initiative—whatever it is—will change the course of history. Really! (And you need to know, I rarely use exclamation points. For this however, I make an exception. So there.)
Sadly, unless we want to recreate fundraising and development terminology, we're stuck with the dry, "Case for Support." What we can do however, is give the document itself some pop, some excitement. When we do, those who are thinking about joining our financial team will notice. We will build stronger relationships, and those we serve will be the ultimate beneficiaries of new financial gifts.
This month's issue then, is about ways we can give this document something extra, and why. In addition, let's look at some new recipients for this document. We might find that the Case for Support (CFS) can make all the difference in an exciting development plan for our ministry.
Click here for more of this month's Advancement Trends in the Life Community.
Our CFS is a Big Deal: A Q & A
by Kirk Walden, Advancement Specialist
Our Case for Support can be a huge boost to our development plan, if we maximize its potential for reaching our financial friends in the ministry. Let's take a look at some questions that will help us identify an effective CFS and how it can make a difference for us in 2015:
What is a Case for Support (CFS), and why do we need one?
By definition, a CFS is a document outlining the reasons why your ministry is important and lays out a plan for the future and/or a specific initiative which needs funding. In most cases, a CFS contains an individual ask for funding the organization or the initiative.
It is a smart idea for every organization to create a CFS whenever a major new initiative is rolled out ("Major" might mean an initiative with a price tag of $25,000 or more), or each year—as a way of sharing with its supporters the plans for the coming 12 months.
How many pages is a typical CFS?
We will look at the key elements in another article ("Core Elements of a Winning CFS"), but this document will likely end up with anywhere from 8-12 pages. Keep in mind, every element needs to be concise. We need plenty of white space in our CFS, to give our friends a chance to glance. We don't want to take them on a literary journey.
Who should receive a copy of our CFS?
If our CFS is primarily referencing a major initiative (expanding our medical ministry, renovations, the purchase of a new property, etc.), the CFS goes primarily to those who can give larger gifts (of $500 or more).
If our CFS is designed to put forth our annual plan, we will not only place it in the hands of major supporters, but we should strongly consider sending it to our monthly supporters, too. The cost is just a few dollars to send this to our monthly supporters but, with a strong thank you letter inside the front cover, it is a strong investment in building a long-term relationship (See our "CFS Thank You Letter" in this issue).
Click here for more of this month's Advancement Trends in the Life Community.
Two Quick Keys to a CFS that Captures Attention
by Kirk Walden, Advancement Specialist
What's our most important goal for our Case for Support (CFS)? Getting people to read it.
Like our newsletter or E-blasts, if no one reads these documents, the news we want to disseminate goes nowhere. What are some characteristics then, of a CFS which garners attention and readership?
Concise articles
As an example, every CFS should contain a "History" page that walks readers through where the ministry has been. Use creative writing sparingly; use bullet points often. Consider two examples:
The AAA Pregnancy Center started in 1984, in the living room at the home of Bill and Mary Jones. There, a prayer group began gathering, praying about a way to address the abortion issue in a Christian fashion. At the meeting were 12 interested people, though more wanted to come. Two weeks later all would meet again and begin planning to create a ministry and obtain 501c3 status for our organization.
Or this:
June 4, 1984—AAA Pregnancy Center's history begins with a meeting of 12 friends at the home of Bill and Mary Jones in Leighton Valley.
May 14, 1985—Our first client arrives on opening day at our first location: 284 Elm Street in Leighton Valley.
March 12, 1986—It's a boy! Jacob is the first child born to a AAA client. Today he is 27 years old; he and his wife have two children of their own.
January 9, 1989—AAA moves into a new home on Main Street. This location would serve us for 19 years.
In the first example, we see a paragraph with mostly superfluous information. The reader is already tired, and likely will not move on to further information on our History page.
In the second, we use almost the same number of words to communicate four milestones. With a bit of detective work, we might find fascinating information that will encourage and bring life to the entire ministry.
Photos
As a writer this is hard to admit, but our readers are drawn more to our photos than to our stunning prose. Those who support us want to see what we are doing, and photos are an excellent way to tell our story. We don't need professional photographers (though this would be great). We do need photos—that tell a story.
Tweet this! It is often more effective to show one client hugging her baby than it is to show fifty clients in a group photo.
It is often more effective to show one client hugging her baby than it is to show fifty clients in a group photo. The photo of one client tells a story; fifty faces is just another group shot.
In addition, use photography to highlight new initiatives, such as construction and renovation. Architectural drawings of new construction can be helpful, too.
Click here for more of this month's Advancement Trends in the Life Community.
Core Elements of a Winning CFS
by Kirk Walden, Advancement Specialist
What goes inside a Case for Support? You can add more than the following, but here is a good start:
Cover Letter
Personalize a letter to the recipient, thanking your financial partner for reading, briefly outlining the reason for the CFS and giving a short overview of the projects or initiatives inside. This letter is less than a page. Say thanks, tell 'em why, and tell 'em how. That's it.
History
A brief, bulleted list of milestones, recognitions and key staff changes ("Myra Jones joined the PRC as CEO, beginning a 12-year tenure that would bring our ministry into the medical realm").
Where we are
Let your friends know what you are accomplishing today. Make sure results are measurable. Our readers will pick up on attempts to be vague in our assessments. Consider two sentences; which is more effective in telling our story?:
One attempt: "We are seeing a lot of clients and they are telling us how much they appreciate what we do for them!"
Or, "A whopping 87% of our clients say they would recommend us to friends. In addition, a documented 83% of those who come to us considering ending their pregnancies ultimately choose life for their children."
A clear picture of why we are asking
Whether the CFS is for a specific initiative or for overall funding, create a clear image for readers of the ministry's needs. "We need more funding for advertising" is not clear.
Instead, try, "Our Outreach Initiative includes $14,400 for a more powerful web presence, $5,845 for signage on our city's main artery, Highway 000, and $4,200 for TV ads on several cable channels that reach our main demographic of 18-24 year old women." Your plan can include even more details, but you see the point.
Give actual numbers. Providing details (keep it concise, but details matter) shows good stewardship and careful planning. Both of these characteristics connect positively with those who can give to you.
A clear appeal
Except for those times when a CFS is sent as purely an informational piece for current donors, Ask. People are always more likely to give when asked. Best-selling author Nora Roberts has some words of wisdom here: "If you don't ask, the answer is always No."
Ways to Give
Tweet this! When it comes to clarity, "Ways to Give" must be at the top of our list.
When it comes to clarity, "Ways to Give" must be at the top of our list. No ask is complete without the "How" portion, and Ways to Give shows our friends specific opportunities to support the ministry.
Here are a few to keep in mind:
One Time Gift—Make sure a return envelope and response device are included with your CFS. Make sure online giving is presented, with your donation site prominently shown. Then check the web site and attempt to make a gift online. Experience it yourself and make sure it is easy.
Monthly Giving—Provide an opportunity to make a monthly (open-ended; not for just one year) commitment. Present this on your web site as well.
Stock Gifts—Explain how to make a stock gift. For more information on this, search the subject online. You will find verbiage and information from universities and major non-profits.
Gifts of Property—Why not present this option as well? Write, "If you would like to make a gift of property to (name of ministry) email Jane Johnson at This email address is being protected from spambots. You need JavaScript enabled to view it. or call her (000-0000) for more information." The more opportunities we present, the better the perception in the donor's mind.
Memorial/Honorarium Gifts—Your response device should present opportunities for Memorial Gifts (honoring those who have passed away) and Honorarium Gifts (Honoring those still living). A large percentage of donors utilize these gift avenues. Let's make them available.
Click here for more of this month's Advancement Trends in the Life Community.
Cover Letter for Our Case For Support
Reaching our monthly supporters
Your Case for Support can be sent to your monthly supporters as a way to keep them informed and invested in the ministry. The following is a cover letter to introduce this document to your monthly supporters. This letter is geared toward a 2015 Annual Plan:
Dear Joe and Jane,
Each month you invest in (name of ministry), making you a vital part of our team and a catalyst in our bright future.
Inside this packet is our 2015 Vision, a look at where we have been, where we are and where we are headed in the coming you. We wanted you to have this report so you could see that your investment continues to change the lives of those who come in our door.
Thank you for your belief in the mission of (name of center) and your commitment.
Together we are saving lives, and changing lives every day. It is an honor to serve alongside you in this mighty work!
Sincerely,
CEO Board Chair
by Kirk Walden, Advancement Specialist
Click here for more of this month's Advancement Trends in the Life Community.
Click here to download this cover letter as a word document.